Understanding Stakeholder Perspectives in Preventing Hospital-Acquired Infections (HAIs)
Preventing hospital-acquired infections (HAIs) is a complex process that involves many stakeholders, including but not limited to:
Babies
Families
Frontline Care Providers
Clinical Leaders
Infection Control Departments
Quality and Safety Departments
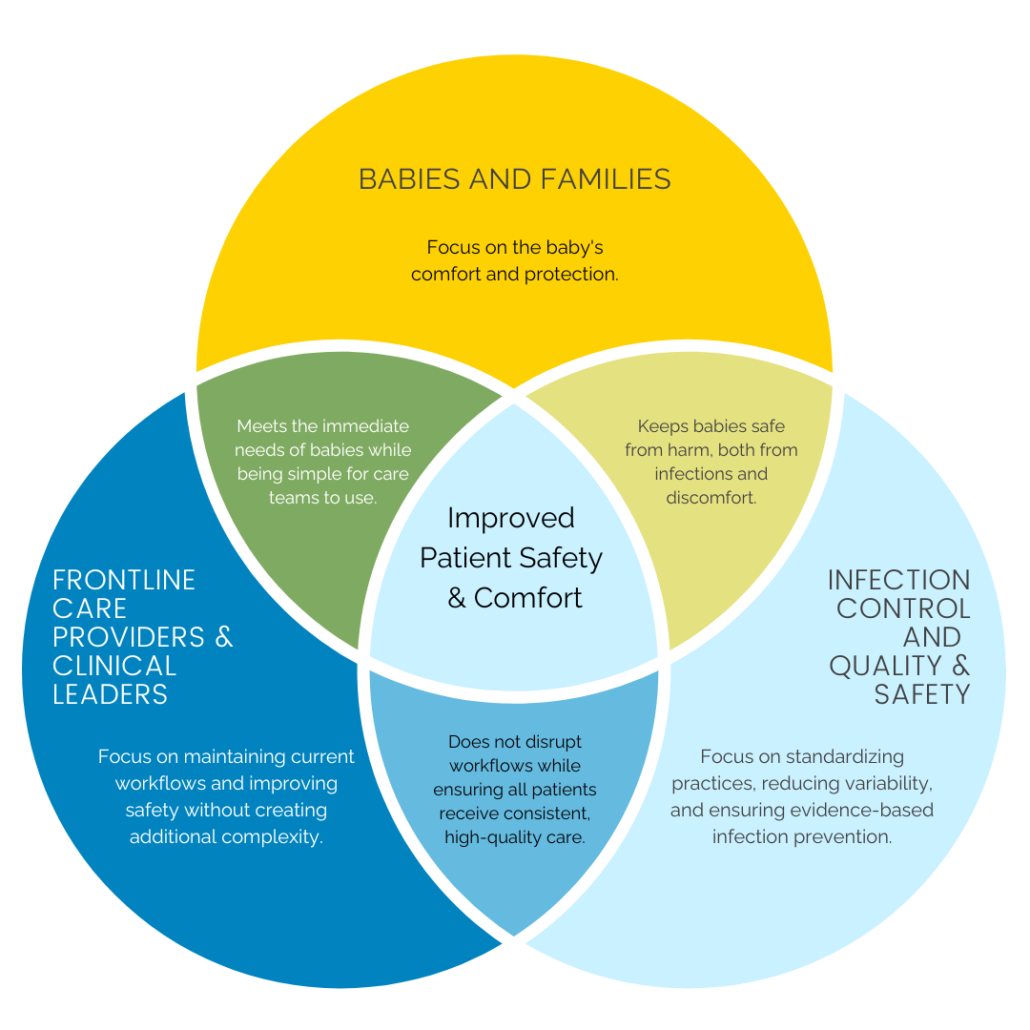
Each of these groups has a shared goal: improving the quality of care for every baby. While their priorities may vary slightly, they all aim to protect patient well-being and prevent infections during hospitalization.
When implementing practice changes, such as introducing new products or procedures, it’s essential to stay focused on the ultimate goal: infection prevention and the baby’s overall health and safety. However, effective communication with each stakeholder requires framing the conversation around their unique perspectives. In this edition of the Dandy Blog, we explore how DandlePURE addresses the needs of these groups while contributing to improved patient outcomes.
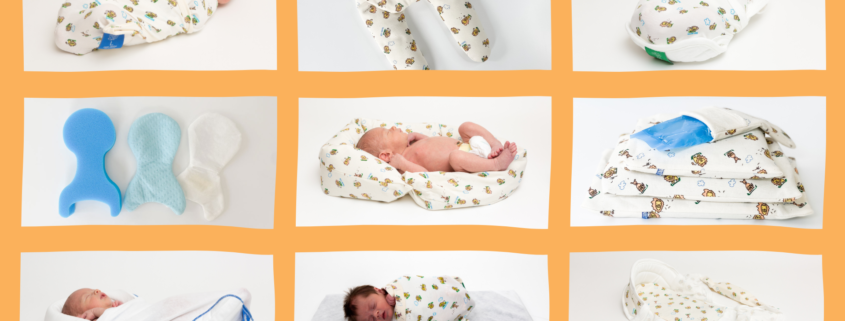
Babies & Families: Comfort and Safety Above All
For families with hospitalized babies, infection prevention, comfort, and safety are the top priorities. DandlePURE mattresses are designed with all three in mind. Made of viscoelastic memory foam, the mattress gently supports babies, redistributing pressure away from bony prominences, promoting restful sleep, and ensuring comfort in any position.
The mattress meets Safe Sleep recommendations, providing a firm sleep surface while remaining pliable enough to support babies in various sleeping positions. In addition, the advanced technology integrated into the PneumaPure® filter, Safeweld® hermetically sealed seams, and Pureshield™ waterproof fabric guarantees that the mattress remains free from contaminants like bacteria, viruses, and allergens, both inside and out. Parents can rest easy knowing their babies are not only comfortable but also protected from potential harm through improved infection prevention measures.
Frontline Care Providers and Clinical Leaders: Simple, Seamless Protection
As discussed in our previous blog post, successful product and practice improvements should simplify clinical workflows rather than complicate them. DandlePURE mattresses seamlessly integrate into existing processes, offering built-in infection protection for babies without adding extra steps for the care team.
This simplicity also benefits clinical leadership. By avoiding unnecessary workflow changes, DandlePURE helps maintain efficiency while supporting safety goals. Clinical leaders are deeply invested in preventing HAIs and rely on consistent, evidence-based solutions. DandlePURE delivers that certainty by ensuring each mattress is free from internal contaminants, reducing the variability that can contribute to infections.
Consistency in products and practices directly enhances patient safety and improves patient outcomes—goals shared by all clinical teams.
Infection Control and Quality & Safety Departments: Standardizing Care for Better Outcomes
Patient outcomes are the central focus of infection prevention, Infection Control, and Quality and Safety teams. These teams are dedicated to implementing the latest evidence-based products and practices to prevent, identify, and respond to HAIs. They are particularly concerned with standardizing care and reducing variability in the hospital environment.
DandlePURE helps achieve both of these objectives by setting a new standard for what constitutes a “clean” patient bed. With the mattress’s advanced contamination-proof technology, these teams can have greater confidence that it is not contributing to the spread of infections. By reducing variability and improving standardization, DandlePURE supports these departments in their mission to protect patients from harm.
Conclusion: A Unified Goal for Better Patient Care
Though their priorities may differ slightly, all of these stakeholders are united in their commitment to improving patient safety and outcomes. DandlePURE is a solution that meets each group’s unique needs, ensuring that every baby receives the highest standard of care while helping hospitals reduce the risk of infection and improve environmental cleanliness.
https://dandlelionmedical.com/wp-content/uploads/2025/03/DandlePURE-Blog-FeaturedImage-6.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2025-03-11 13:43:552025-03-19 11:32:31DandlePURE: A Solution That Works for NICU Teams, Infection Control, and Beyond
Hospitals are becoming increasingly complex, with higher patient acuity, greater reliance on technology, and increasing demands on clinicians. Healthcare facilities are tasked with balancing innovation with practicality—ensuring that new products and solutions enhance safety without adding complexity to already burdened systems. As responsibilities grow, so does the challenge of maintaining a clean and controlled care environment while ensuring that every patient receives the safest care possible.
One of the greatest obstacles in infection control is managing the variables that contribute to healthcare-acquired infections (HAIs). Some factors—like breaches in line integrity—are easily identified and addressed. But others—like environmental cleanliness—are highly variable, difficult to control, and even harder to improve.
The Human Factor in Infection Control
The finite capability of humans to adequately respond to increasing demands while continuously adjusting their behavior presents a particularly challenging scenario in healthcare. Our greatest strength—our humanity—can also be our greatest vulnerability. As the saying goes, “To err is human.”
It is incumbent upon healthcare facilities to make mindful decisions about improving practices, purchasing products, and implementing projects that facilitate positive change without overstraining existing systems of care. Facilities must strategize and simplify ways for their employees to carry out necessary changes consistently, acknowledging the limitations of being human.
Ideally, improvements in care practices, products, or processes increase safety and quality of care without placing additional demands on clinicians—allowing them to focus on what matters most: caring for their patients.
A Mattress That Helps Protect Infants & Caregivers
One area where this balance is especially critical is infection control. Despite strict cleaning protocols, traditional hospital mattresses can absorb fluids, harbor pathogens, and introduce unseen infection risks. When an infection occurs, root cause analysis often focuses on known factors, such as breaches in protocol. However, unknown environmental contributors, like contaminated soft surfaces, remain difficult to identify and even harder to control.
Soft surfaces in hospitals have long been recognized as potential reservoirs for pathogens, yet for decades, neonatal units lacked a better alternative—one that provides both proven pathogen resistance and easy maintenance. Until now.
DandlePURE: A Mattress Designed for a New Standard of Clean
Enter Dandle®PURE Neonatal Mattresses—a simple and effective way to improve care and decrease variability in environmental cleanliness without increasing caregiver burden.
DandlePURE Neonatal Mattresses provide a simple, effective solution to this ongoing problem. Unlike traditional hospital mattresses that allow pathogens to accumulate over time, DandlePURE offers next-level infection control through:
By integrating sealed barrier technology and an advanced filtration system, DandlePURE helps hospitals reduce infection risks, decrease variability in environmental cleanliness, and ensure a more consistent standard of care.
As healthcare evolves, facilities must continue to seek innovative solutions that improve patient safety without overburdening staff. We want hospitals to strategize smarter, simplify infection control, and build safety directly into the care environment—without increasing the demands on their already stretched teams.
DandlePURE isn’t just a better mattress—it’s a better foundation for infection control.
https://dandlelionmedical.com/wp-content/uploads/2025/02/DandlePURE-Blog-FeaturedImage-1.jpg10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2025-02-19 15:17:402025-02-19 16:56:41DandlePURE: The Neonatal Mattress That’s Raising the Bar in Infection Control
Lori Brittingham is a Neonatal Clinical Nurse Specialist and Dandle•LION Clinical Consultant with over 30 years of NICU experience. Having spent over 25 years at The Children’s Hospital of Philadelphia, she played a key role in developing neurodevelopmental care and small baby teams in the Level 4 NICU.
With recent roles at Reading Hospital-Tower Health in Pennsylvania and Nemours Children’s Health in Orlando, FL, Lori focused on aligning clinical practice with evidence, enhancing quality and safety outcomes, and advancing the clinical nurse specialist role. A former adjunct faculty member at the University of Pennsylvania School of Nursing Science (2014-2019), she holds a BSN from Temple University and an MSN from the University of Pennsylvania.
Lori served on the National Association of Neonatal Nurses board for 8 years, including a term as President (2016-2018). Recognitions include CHOP’s Nursing Leadership Award (2014), the Pennsylvania Nightingale Advanced Practice RN Award (2018), and the National Association of Clinical Nurse Specialists’ Clinical Nurse Specialist of the Year Award (2019). An inaugural recipient of NANN’s Developmental Specialist designation, Lori played a pivotal role in the inception and execution of this important recognition program.
Dandle•LION is proud to partner with expert clinicians to provide the best available education and evidence-based care strategies. We are excited to introduce you to Emily Hills, MSc, CNT, NTMTC, NIDCAP, a Clinical Specialist Neonatal Occupational Therapist at Starlight Neonatal Unit, Barnet Hospital, Royal Free London, NHS Foundation Trust!
Emily leads developmental care, neurobehavioral, neurodevelopmental, and sensory assessment, and interventions— including follow-up after discharge.
Emily is a certified neonatal therapist (CNT). She has completed her MSc in Advanced Neonatal Studies at Southampton University. Emily is NIDCAP certified and lectures on The Family and Infant Neurodevelopmental Education (FINE) program in the UK. She is a senior Brazelton trainer and is certified to teach on the Newborn Behavioral Observation (NBO).
Emily is a co-author and co-founder of Sensory Beginnings Ltd and is an Advanced Practitioner in Sensory Integration (SI). Emily has completed Neonatal Touch and Massage certification (NTMC) and has completed the advanced course in The Prechtl General Movement Assessment.
Links & Resources
Hills, E., Hynard, L., Deierl, A., Aloysius, A. & Harding, C. (2023). Enhancing therapeutic support for inpatient infants and families by introducing Lullaby Hour to the neonatal unit. Infant, 19(2),
Gupta N, Deierl A, Hills E, Banerjee J (2021) Systematic review confirmed the benefits of early skin to skin contact but highlighted lack of studies on very and extremely preterm infants. Acta Paediatrica; 00:1-6
Hills E, Harding C (2020) A multidisciplinary approach to the implementation of non-pharmacological strategies to manage infant pain. Infant; 16(2): 78-81.
Harding C, Mynard A, Hills E (2017) Identification of premature infant states in relation to introducing oral feeding Journal of Neonatal Nursing 24 (2)
https://dandlelionmedical.com/wp-content/uploads/2024/08/Emily-Hills-Clinician-Spotlight-BLOG.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2024-08-27 15:43:082024-08-27 15:43:09Clinician Spotlight: Emily Hills, MSc, CNT, NTMC, NIDCAP
“Hospitalized preterm infants should be placed supine as soon as clinical status has stabilized and they have achieved positional stability, that is, when therapeutic or non-supine positioning is no longer medically indicated. This milestone is usually achieved by 32 weeks’ gestational age.”
(AAP, 2022).
Following the recommendation of the American Academy of Pediatrics (AAP) (Committee on Fetus and Newborn, 2022), many NICUs enact Safe Sleep parameters at around 32 weeks postmenstrual age, which often involves removing all developmental positioning supports in an effort to model Safe Sleep for parents.
Although implementing back to sleep as early as 32 weeks postmenstrual age is recommended, it is important to consider the musculoskeletal and sensory organizational processes occurring in the infant between 32 weeks and term gestation. These factors should be considered when determining “positional stability”:
Development of physiologic flexion posture as the foundation of normal motor development matures in the last weeks of pregnancy.
Joint compression and resistance to active extension necessary for bone development is most prevalent in the last trimester of pregnancy.
Calcium and phosphorus acquisition for bone ossification is maximized in the third trimester of pregnancy.
The degree of prematurity directly affects an infant’s ability to maintain positional stability secondary to medical equipment required to support respiration and digestion, immaturity or atypical development of the central nervous system requiring cardiopulmonary monitoring, and possibly delayed skeletal maturation.
When determining “positional stability,” each infant’s medical and developmental needs should be considered before removing developmental positioning supports at a predetermined gestational age. Choosing a wearable blanket or swaddle that promotes flexion of the extremities provides dynamic support, allowing free movement while promoting passive recoil to a flexed posture is a reasonable option that supports positional stability and meets the AAP guideline for Safe Sleep. This dynamic relationship between baby and boundary is an essential component of healthy physical and sensory development.
Developmentally speaking, removing positioning aids early in the 3rd trimester may deprive the baby of the increasing physiologic flexion they would have experienced in the womb, which is vital to bone and muscle development.
A 32-week infant, for example, should still experience an additional 6-8 weeks of pregnancy before neurologic and physical development are optimal. However, not every 32-week infant is the same physiologically or neurodevelopmentally.
A 32-week baby born at 24 weeks gestation may have dramatically different physical and sensory support needs than a 32-week baby born at 31 weeks gestation.
Babies born at earlier gestational ages with more severe illnesses or congenital anomalies may require robust developmental support beyond reaching full term, making traditional swaddles and wearable blankets ineffective in meeting their needs.
Positioning with Purpose
In the third trimester, the “resistance training” provided by the baby’s interaction with the dynamic, muscular boundary of the uterus facilitates proper development of the bones, muscles, and joints. Preterm infants are born prior to the completion of the third trimester, placing them at risk for altered physical development.
Research evidence demonstrates that active resistive movement is essential for skeletal development along with maximized infant nutrition.
The interaction between the baby and the muscular-responsive uterus is essential in loading bones sufficiently to maximize bone accretion.
During this formative period in pregnancy, an exponential increase in bone growth occurs, resulting in 80% of fetal bone being produced (Drake, 2022).
In utero, especially in the last trimester, babies are increasingly flexed within a confined space. The confined boundaries are dynamic in nature and, along with a flexed posture, serve specific purposes in physical and neurological development: • Bone loading to optimize bone accretion • Muscle development • Self-regulation and calming
The Dandle® WRAP Stretch provides dynamic resistance to extension movements of the extremities while promoting the return to a flexed resting posture, mimicking the action of the uterus:
Flexion and midline alignment of the infant in the womb is important for developing bones, joints, and muscles. This posture also facilitates self-regulation and calming, physiologic functions like digestion, and attainment of future motor milestones like rolling, crawling, and walking. Only when an infant can maintain this posture should they be considered as having obtained “positional stability.”
Commercially available swaddles and sleep blankets generally allow for free movement, but when applied to preterm infants in the NICU, they often do not provide recoil or promote a consistently flexed, midline posture— leaving the lower extremities unsupported in extension.
As the Dandle WRAP Stretch is secured under the baby’s head and neck, it meets the definition of a wearable blanket/sleep sack, meeting both the safety and developmental needs of the infant. The physiologic importance of continued developmental support into the third trimester is clear. Providing babies with dynamic support by using a Dandle WRAP Stretch supports the infant’s musculoskeletal and sensory organizational needs while meeting the AAP 2022 recommendations.
The Dandle WRAP Stretch aligns with AAP Safe Sleep recommendations by having no loose fabric or parts around the baby’s airway. It is made of a breathable, three-way stretch fabric that provides close-fitting containment without potentially contributing to overheating. We simply recommend transitioning to a home-like sleep support around 1-2 weeks prior to discharge in order to give the baby time to adjust to what sleep will feel like at home. The Dandle WRAP Stretch can be used until that time.
Dandle•LION supports modeling Safe Sleep while encouraging hospitals to keep babies in their positioning aids for as long as possible within the context of their own unique policies/procedures around safe sleep. Our Dandle WRAP Stretch is compatible with AAP Safe Sleep recommendations and can be used even after “safe sleep” protocols have been implemented for a particular patient.
Drake, L. (2022). Positioning the neonate for best outcomes. National Association of Neonatal Nurses.
Shea, C.; Rolfe, R.; and Murphy, P. The importance of foetal movement for coordinated cartilage and bone development in utero. Cone Joint Res, 2015: 7:105-116. Doi:10.1302/2046-3758.47.20000387.
https://dandlelionmedical.com/wp-content/uploads/2024/06/BLOG-Promoting-Safe-Sleep-Featured-Image-1.png6281200dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2024-06-24 08:58:402024-07-09 09:39:41Promoting Safe Sleep while Protecting Neurodevelopment: The Dandle® WRAP Stretch
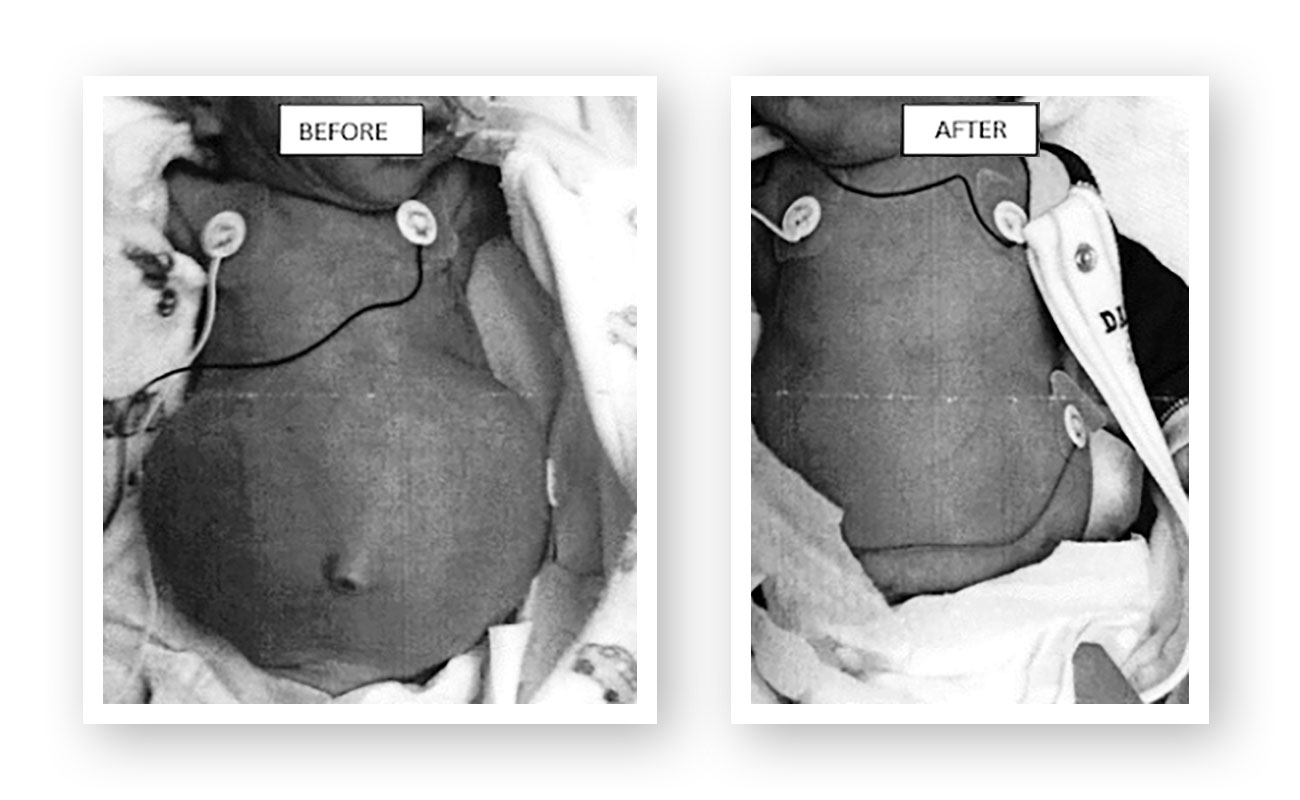
Continuous Positive Airway Pressure (CPAP) is a widely used respiratory support for preterm infants. However, concerns about abdominal distension due to CPAP, often referred to as “CPAP belly,” have sparked discussions about its potential sequelae and called for innovative solutions.
As a physical therapist working in NICUs for over 20 years, I have seen the miraculous work done to save the lives of premature infants. Neonatal therapists often enter this environment with an eye toward addressing or preventing the consequences of prematurity. From positioning in flexion rather than flat on a bed to modifying the environment to meet the needs of immature senses, many simple ideas have improved the care of these infants.
When observing bellies bloated by CPAP, I saw muscles that were stretched outside of their effective line of pull, placing the musculoskeletal system at a disadvantage to take over respiration after CPAP was removed. I saw arching and discomfort. This led me to embark on a journey to address and possibly prevent this unintended consequence of respiratory support.
The first attempts were on older infants to rehabilitate their weak abdomens after CPAP had been discontinued. The first trial involving half-time wear of an abdominal support resulted in these changes:
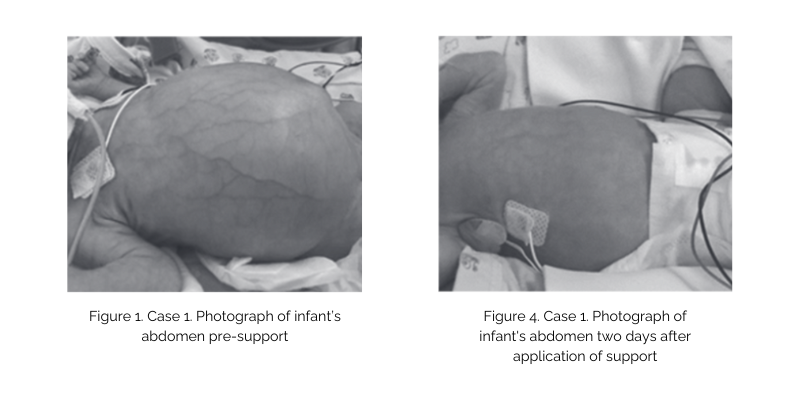
This inspired further work, development of safety criteria, and trying on younger and younger babies to work towards prevention of CPAP belly. Prevention hoped to not just preserve muscle length and function but also to avoid the escalations in support sometimes used to try to overcome the respiratory inhibition which results from air in the GI system. I published two cases, one of treatment and one of prevention. When presenting these cases at a conference, it was clear this is a common issue from the line of therapists who stayed to discuss this further.
As one therapist in Anchorage, Alaska, with a simple idea, how do you help all these therapists? We are taught to communicate our work by publishing and presenting, and I had done that. And while I continue to gather data and prepare for further publication, it was obvious therapists were seeking support to help infants in their units. Some had already tried with different materials and differing success. I had done the groundwork, now how to get consistency in use for all these different units?
Source: McGill, V. (2022). Neonatal abdominal support to address CPAP Belly: Two cases report and literature review. Journal of Neonatal-Perinatal Medicine; 831-836. doi:10.3233/NPM-221047.
I am grateful Dandle•LION has been a partner in this cause. As a wise friend once said to me, you can do anything, but you can’t do everything. With a mind to provide consistency and safety for further use and study, the NeoBellyBand was born. Product development allows us all to know we are using what was used through the years of my CPAP belly journey and to know further study is all testing the same thing done the same way.
During this ongoing journey, the list of concerns about gaseous distension I hear from clinicians continues to expand. I started with weakness and concern for postural support for respiration now and movement development later. Those concerns expanded to the acute complications of distension during respiratory support, like the need for escalation of support to overcome a big belly. Others have expressed concerns about GI complications from feeding tolerance to SIP and still others the long-term consequences of visceral distension on digestion and possibly leading to ongoing inflammation.
These journeys take time, and all begin with one step. And while mine started on my own with a simple idea, it takes a team to make change. Thanks to Dandle•LION and all the clinicians I have spoken with since sharing this idea, who all hope to continue this journey towards improving the care of premature infants.
You are welcome to visit neophysicaltherapy.com to learn more and participate in the conversation, including what parents are saying.
by Ginny McGill, PT, DPT, CNT, NTMTC
Ginny McGill graduated from Creighton University with a Doctorate in Physical Therapy in 2001. She has practiced in the NICU for 22 years, at Phoenix Children’s Hospital and Providence Alaska Children’s Hospital. She has received certifications in Neonatal Therapy, Neonatal Touch and Massage, as well as wound care and lymphedema. Ginny teaches locally and nationally. You may have seen her speak through her work with the Vermont Oxford Network (VON), Engage Grow Thrive, or Creative Therapy Consultants.
https://dandlelionmedical.com/wp-content/uploads/2024/02/Feb-24-NeoBellyBand-Blog-Featured-Image.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2024-02-07 13:44:182024-02-16 22:44:38Are you concerned about abdominal distension?
Vibration is everywhere: in our cars while we drive, on our phones or pagers, in the laundry room from the running clothes dryer, and in the bathroom when the water is running. We even have vibrating toothbrushes. Anything with motion or a motor produces vibration.
Vibrating bouncy seats have long been a home staple for managing fussy newborns. Vibration is shown to ease acute pain, calm children with sensory processing differences, and reduce muscle tightness and spasms. According to the Gate Theory, it interrupts pain transmission in both the afferent and efferent pain pathways.
What about vibration used in the NICU?
According to the study completed by Sequi-Canet et al. (2022), the NICU incubator alone provides a constant source of vibration. High-frequency ventilators such as the Jet and oscillating ventilators also produce constant vibratory input to the infant. Several studies have shown how vibration at the site of the painful prick for blood collection can reduce the pain experience significantly.
Vibration has been used in pediatric to neonatal ICU to reduce the distress of neonatal abstinence and neonatal opioid withdrawal. Zuzarte et al. (2017) demonstrated the effectiveness of vibration for NOWS symptoms, while Smith et al. (2015) demonstrated the regulatory effect of vibration on apnea and bradycardia in the newborn population. Vibration that is applied appropriately has become an effective pain management strategy in dentistry, intensive care, and the emergency room.
Vibration can be applied locally using a small vibrating tool, or across the body using a vibrating mat. Dandle•LION Medical provides the Tranquilo® Soothing Mat for this very purpose. There are several optional protocols for vibration use in the NICU. Protocols should be created from the literature evidence and hospital policies for safe equipment use.
References:
Smith, V; Kelty-Stephen, D.; Ahmed, M; Mao, W; Cakert,K.; Osborn, J.; Paydarfar, D. Stochastic Resonance Effects on Apena, Bradycardia and oxygenation: a Randomized Control Trial. Pediatrics (2015) 136 (6): e1561 – 1568. https://doi.org/10.1542/peds.2015-1334.
Sequí-Canet JM, Rey-Tormos Rd, Alba-Fernández J, González-Mazarías G. Vibroacoustic Study in the Neonatal Ward. Healthcare. 2022; 10(7):1180. https://doi.org/10.3390/healthcare10071180.
Zuzarte I, Indic P, Barton B, Paydarfar D, Bednarek F, Bloch-Salisbury E (2017) Vibrotactile stimulation: A non-pharmacological intervention for opioid-exposed newborns. PLoS ONE 12(4):e0175981. https://doi.org/10.1371/journal.pone.0175981.
Elizabeth is a Clinical Consultant for Dandle•LION Medical and the Developmental Specialist and Neonatal Therapist in Neonatal Intensive Care at Sandford Children’s Hospital/USD Medical Center in Sioux Falls, South Dakota. Read more about Elizabeth in her Dandy Clinician Spotlight.
https://dandlelionmedical.com/wp-content/uploads/2023/09/Guide-Dimensions.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2023-09-06 12:03:122023-09-08 12:12:28What’s The Buzz About Vibration?
Sweet Cheeks® 40% Glucose gel— specifically designed for neonates, benefits babies and clinicians.
Glucose Gel Use In Neonates
40% glucose gel has been demonstrated in the literature as an effective means of stabilizing blood glucose levels in the early newborn period for certain neonatal patients. By reducing the need for IV dextrose, the use of glucose gel in certain neonates has been shown in clinical studies to:
Decrease length of stay
Reduce admissions to neonatal intensive care units
Decrease total costs incurred by patients’ families
Glucose gel has also been shown in clinical studies to have a positive impact on the percentage of babies consuming a 100% human milk diet by decreasing the need for formula supplementation. Other clinical studies have shown that glucose gel is simple to use, well-tolerated by infants, and may allow parents and babies to stay together in the post-birth period.
Risks & Limitations of Commonly-Used Formulations
Historically, commercial glucose gels labeled for over-the-counter use in children over the age of two or adults have been repurposed for use in neonatal units. This method is not without risks and inefficiencies. The amount of glucose gel within a typical commercially available container far exceeds what is needed for neonatal administration. Facilities must therefore either repackage the gel into smaller containers, introducing the potential risk of contamination during transfer and decreasing the efficiency of clinical workflows or discard the excess glucose, potentially resulting in financial waste.
In commercial pediatric and adult preparations, uneven distribution of glucose within a single tube has been found in clinical studies. Glucose gels intended for pediatric or adult use are often intended to be ingested all at once, making any differences in concentration throughout the container less concerning in those populations. However, taking small aliquots from the same single over-the-counter container to administer the gel to neonates presents a risk of variation among the aliquots, potentially impacting the percentage of glucose received by each baby. This could unintentionally lead to variability in clinical response to the intervention.
A Neonatal Formulation Designed to Improve Efficiency & Reduce Waste
The apparent risks associated with using over-the-counter pediatric and adult glucose gels for neonates have largely been tolerated by clinicians due to the lack of a viable alternative. To address this important need, Dandle•LION Medical developed Sweet Cheeks 40% Glucose Gel.
Sweet Cheeks is packaged inside an oral syringe in 3mL aliquots, making the administration of neonatal glucose gel simple and efficient with no age limitations. After verifying the ordered amount of glucose gel, clinicians simply squeeze out the excess gel, leaving only the gel needed for their patient. The gel is then squeezed onto a clean, gloved fingertip and applied inside the buccal cavity for direct absorption into the bloodstream.
To request a sample of Sweet Cheeks 40% Glucose Gel, please click here.
https://dandlelionmedical.com/wp-content/uploads/2023/06/Guide-Dimensions-3.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2023-06-14 15:39:322023-06-15 11:27:55Isn’t It Sweet? 40% Glucose Gel Made Just For Babies
Our PAL Family consists of the Dandle® PAL, Polly PAL™, and the Mini PAL™! All three are weighted positioning aids that provide multiple uses during a baby’s stay in the NICU. Keep reading to learn about what makes each member of the family unique.
Mini PAL™
Say hello to the youngest member of the PAL Family!
The Mini PAL (right) is next to the Dandle PAL for size reference.
The Mini PAL was designed specifically for the tiniest babies that need more support inside the extra small Dandle® ROO2 and ROO Lite.
Like her older brother and sister, Mini PAL is a flexible positioning aid that can be used in a variety of ways:
A tool for supporting medical equipment while taking up minimal space
An insert in the XS Dandle ROO2 or Dandle ROO Lite to fill in space at the bottom so the wings and pouch fit properly
A lightweight positioning accessory placed gently alongside the baby with the “legs” laid over the baby’s shoulders, hips, or behind the head
The Mini PAL has an outer and internal bag filled with silky micro discs and is currently available in a machine-washable version.
Coming soon for Mini PAL: a wipeable version with disposable and washable cover options!
Dandle® PAL
The Dandle PAL is a flexible boundary with dual-weighted pouches that can be easily nestled around an infant to provide containment and support.
Washable Dandle PAL (left). Wipeable Dandle PAL (right).
The larger pouch comprises the “legs,” which provide support and flexion, while the smaller pouch gives height or extra support when needed. The unique twill tab allows clinicians to stack the two compartments over one another and secure them in place, providing stability and height where it’s needed most. The silky micro discs can be shifted to personalize care.
The Dandle PAL serves a variety of additional functions:
Acts like a “second set of hands” to comfort the baby during patient care
Holds medical devices in place to reduce the likelihood of malposition, unintended removal, or pressure injury
Supports upper and lower extremities simultaneously when used in pairs
This product has a washable and wipeable version, along with disposable and washable covers for the wipeable Dandle PAL.
Polly PAL™
The Polly PAL.
The Polly PAL is a smaller, single-bag weighted boundary that supports positioning in the NICU.
This boundary also serves a variety of functions:
Around the head to encourage midline positioning
Supports respiratory equipment or other medical tubing
Behind the back, when the baby is side-lying
A “second set of hands” to provide comfort during patient care
Anywhere the baby needs a little bit more comfort or support
https://dandlelionmedical.com/wp-content/uploads/2023/04/V2-The-PAL-Family.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2023-04-11 13:30:482023-12-18 13:28:21The PAL Family
Commonalities exist in providing developmentally-appropriate support to babies in the NICU, CVICU, and PICU, particularly in managing:
Posture
Position
Pain
Sleep
One intervention common across these areas is head of the bed (HOB) elevation.
Elevation aids digestion and secretion management, and reduces ventilator-associated pneumonia; a serious complication regardless of age. Elevation can also be important in post-surgical recovery.
The challenge presented with HOB elevation is the tendency for the infant to slip down the mattress.
Preventing Infants From Slipping Down The Mattress
Weighted Boundary
The infant will often roll, twist, or slide down the incline. Positioning techniques can reduce this migration through the use of physical support (such as a weighted boundary) combined with a comforting, developmentally-appropriate posture.
Baby pictured in a weighted boundary that provides proprioceptive feedback.
A weighted boundary also supports sleep, calmness, energy conservation for healing, and feelings of security, while reducing pain. There are several ways to support an infant that promote postural symmetry, head rounding, natural body contours, and self-calming. Positional support also provides a tactile cue that nursing cares are complete and it is time to rest.
A large flexible weighted boundary that contours to the child’s body provides:
Reduced migration on the bed surface
Postural support
Full visibility of the baby
Swaddling
Baby pictured in a swaddle wrap to provide dynamic support, with a smaller weighted boundary that provides support to the head.
In situations where full visibility is not necessary a dynamic, stretchy swaddle wrap can be added to provide 360 degrees of comfort through proprioceptive feedback and warmth.
Supportive Accessories
A smaller weighted boundary can be used to stabilize an extremity in extension to allow for proper intravenous catheter function. When asymmetry is present, these smaller boundaries can support the head in midline or head-turning.
Prone Positioner
Baby pictured on a prone positioner to provide a comfortable, flexed posture in the prone position.
In some situations, an infant may need to be placed on their abdomen.
In these cases, a prone support device can ease the alignment of the ventilator tubing and the airway and allow the infant to assume the fetal position with arms and legs tucked close to the body, a typical position of comfort for infants. A prone support device is especially beneficial when caring for an ex-premature infant who still hasn’t reached term gestation.
For the very young infant in the CVICU or PICU, a consistent signal that the cares and all the “owies” are finished for the time being impacts trust building with caregivers and overall cooperation with unpleasant but necessary activities. Multiple strategies exist to support infants in CVICU or PICU.
A note from the team at Dandle•LION:
Dandle•LION Medical offers products that can provide a weighted boundary, dynamic swaddling, and prone positioning. Learn more about the following products:
Elizabeth is a Clinical Consultant for Dandle•LION Medical and the Developmental Specialist and Neonatal Therapist in Neonatal Intensive Care at Sandford Children’s Hospital/USD Medical Center in Sioux Falls, South Dakota. Read more about Elizabeth in her Dandy Clinician Spotlight.
https://dandlelionmedical.com/wp-content/uploads/2023/02/03_03_23-BLOG-FEATURED-IMAGE-Positioning-Babies-In-Critical-Care-1.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2023-02-27 17:15:362023-03-03 15:01:07Positioning Babies In Critical Care
During gestation, babies receive consistent, predictable positioning and sensory input from the womb. Positioning and sensory interventions in the NICU should ideally promote consistency in practice across caregivers, such as using dedicated tools that decrease variability in positioning technique. Having consistent, evidence-based positioning support tools can be viewed as an important step toward improving developmental care.
Our social media series Consistency Is Key covered three main areas of neonatal positioning that benefit greatly from consistent neurodevelopmental support. Find all of the slideshows in one place with additional information about Swaddling, Nesting, and Prone Support below:
Swaddling
Swaddling has been used for centuries to provide babies with warmth and calming containment. Hospitalized babies— especially those born preterm— need consistent, neurodevelopmentally-supportive positioning that aims to bridge the gap between the experience of the womb and the experience of the NICU.
Traditional swaddling with blankets may not provide the right type of support to optimize growth and development. High levels of variation can exist in blanket swaddling techniques, resulting in a variable experience and position for the baby.
Babies also need dynamic boundaries that allow for free movement and periods of active extension, followed by passive recoil to flexion at rest. Traditional blankets may be stiff, preventing free movement and failing to promote recoil to flexion.
An ideal swaddling aid should make it easy to provide the right position and sensations for each baby, without the influence of caregiver preference or technique on the outcome.
Positioning nests crafted, folded, or molded by hand are a long-standing tradition in NICU environments.
While these types of support can be effective with the right technique, the potential exists for high variability in positioning across caregivers, babies, and even shifts.
Nesting with products that provide close-fitting, easy-to-replicate positioning support will give the babies the redundancy and dynamic interplay characteristic of the womb. Womb-like positioning can promote deeper sleep, which benefits babies, their parents, and caregivers alike!
Developmentally supportive prone positioning should facilitate a flexed posture, with the shoulders rounded, hips and knees flexed, and hands toward the face.
Prone supports that are built from blankets, burp cloths, pillowcases, or other flaccid materials may not be firm enough to promote and maintain proper prone positioning.
https://dandlelionmedical.com/wp-content/uploads/2023/01/Guide-Dimensions-2.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2023-01-03 10:53:372023-06-12 13:00:51Consistency Is Key: Neonatal Positioning For Neurodevelopmental Support
Adding a new piece of equipment into the daily routines of NICU baby care is challenging for many reasons; most prominently is a lack of familiarity with the product.
When introducing a product similar to one already in use, staff adjust more quickly. However, when a product is unfamiliar, the transition takes more time. Helping the team become familiar with the new product is vital.
Pictorial Guides
There are many ways to accomplish this goal, but each takes time. For starters, place pictorial information about the product in all the common spaces such as the lounge, scrub station, bathrooms, and group charting areas. Using a picture of the device in use is extra helpful, plus a few bullet points explaining its purpose, population, and process. DandleLION has created a QR code linking the nurse or therapist to the website’s positioning products.
DandleLION offers various pictorial guides and in-service videos for our products on the website to expedite this step in the change process.
Hands-On Interaction & Feedback
Have a product open house! If available, place several product sizes in the staff lounge with general guidelines for use. Allow staff to interact with the products on a doll of different sizes, and allow for open discussion where team members can relay positive and negative attributes. This implementation gives staff hands-on familiarity and increases buy-in when asking to hear staff opinions.
Mini Bedside Education
Offer mini bedside education sessions 5 minutes maximum length. In this “5 minutes to know,” introduce why the product is necessary, how to use it and what benefits its use will yield. Offering a token reward for completion, a sticker for their badge, some candy, or a pen, improves motivation and provides peer pressure to others who see the token and want one too. DandleLION has created a badge card with a picture of each positioner and a QR code linking to the website. The badge card is a great reward and a ready reminder.
Finally, create easy access to the product. Give the product a little front-shelf time, if possible. Make signs guiding staff to the product, and shelve it with other like or same process items such as midline head supports near the admission items. These simple steps can improve the ease of transition and the likelihood of use.
Elizabeth is a Clinical Consultant for Dandle•LION Medical and the Developmental Specialist and Neonatal Therapist in Neonatal Intensive Care at Sanford Children’s Hospital/USD Medical Center in Sioux Falls, South Dakota. Read more about Elizabeth in her Dandy Clinician Spotlight.
https://dandlelionmedical.com/wp-content/uploads/2022/09/09_12_22-BLOG-Integrating-New-Equipment-.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2022-09-12 13:38:512022-09-12 14:49:57Tackle The Challenge Of Integrating New Equipment
In 2011, national legislation was passed designating the month of June as “National Cytomegalovirus (CMV) Awareness Month” and recommending that “more effort be taken to counsel women of childbearing age of the effect this virus can have on their children.” Even though congenital CMV is the leading viral cause of congenital disabilities and the leading non-genetic cause of childhood hearing loss, most adults have never heard of it. The National CMV Foundation was incorporated in 2014 with hopes of changing these statistics. The organization began with a mission to raise awareness and educate women of childbearing age about congenital CMV. A year later, the National CMV Foundation joined forces with three prominent CMV non-profit organizations: Maddie’s Mission, Stop CMV, and the Utah CMV Council to become the largest national advocacy organization focused on congenital CMV. The organization is focused on our vision to eliminate congenital cytomegalovirus (CMV) in the United States for the next generation. We are honored to share information about CMV for National CMV Awareness Month this month.
Farah Armstrong, founder of Maddie’s Mission and co-founder of the National CMV Foundation, and her husband at a Stop CMV Golf event.
What is CMV?
Cytomegalovirus (sy·toe·MEG·a·low·vy·rus) or CMV, is a member of the herpes virus family. Coming into contact with the CMV virus is a common occurrence, typically harmless to the general population. A CMV infection causes cold-like symptoms, such as a sore throat, fever, fatigue, and swollen glands. These mild cytomegalovirus symptoms last for only a few short weeks and are rarely a cause for concern for healthy kids or adults.
It is important to note that the CMV virus can cause serious problems for people with weakened immune systems (immunocompromised) due to organ transplants, HIV/AIDS infection, chemotherapy, and specific medications, such as glucocorticoids, cytostatics, antibodies, and drugs acting on immunophilins.
The CMV virus can also cause severe disease in babies who were infected with CMV before birth (referred to as congenital CMV infection).
According to the Centers for Disease Control and Prevention (CDC), between 50 and 80 percent of people in the United States have had a CMV infection by the time they are 40 years old.
Once the CMV virus is in a person’s body, it stays there for life and can reactivate. A person can also be reinfected with a different strain of the virus.
Healthcare Provider Information and Resources
CMV can be a serious problem for babies who are infected before birth. This is referred to as congenital CMV and it occurs when a pregnant woman passes the virus to her unborn child. Congenital CMV can cause birth defects and developmental disabilities and more children will have disabilities due to congenital CMV than other well-known infections and syndromes, including Downs Syndrome, Fetal Alcohol Syndrome, Spina Bifida, and Pediatric HIV/AIDS. We have provided these resources for physicians, OB-GYNs, midwives, nurses, and clinicians to enable better identification, prevention, and treatment for congenital CMV.
In the United States, approximately 1 to 4% of women will have their first, primary CMV infection during pregnancy, and about 40% of these women who become infected with CMV for the first time during pregnancy will pass the virus to their babies. It is crucial that physicians and OB-GYN doctors share this information with women who are pregnant or preparing for pregnancy.
Looking for guidance on how to best counsel women about congenital CMV during pregnancy? The CDC offers a PDF download titled “CMV Facts for Pregnant Women and Parents” that may be helpful here.
About 1 out of every 200 babies (roughly 30,000 children annually) is born with congenital CMV making it the most common congenital viral infection in the United States. More than 6,000 children annually suffer permanent disability as a result. Severe complications from congenital CMV result in approximately 400 deaths nationwide per year.
Transmission
Transmission of CMV is very rare through casual contact. CMV is spread from one person to another, usually by direct and prolonged contact with bodily fluids, including saliva, urine, and breast milk.
CMV is common among healthy children 1 to 3 years of age who attend daycare and can easily spread CMV among their peers. CMV is not generally harmful to these children and most kids will not show any signs or symptoms of infection.
Contact with the saliva or urine of young children is a major cause of CMV infection among pregnant women, especially mothers, daycare workers, preschool teachers, therapists, and nurses. Women who are pregnant or plan to become pregnant should practice standard hygiene procedures around young children to reduce their risk of CMV infection because the virus can be transmitted to their unborn child.
Signs/Symptoms of CMV in the Pregnant Patient
Most people who contract CMV will show no symptoms and may not even know that they have been infected. Others may develop a mild illness and may have any of the following symptoms:
National CMV Foundation’s Stop CMV Golf event.
High fever
Fatigue
General discomfort, uneasiness, or ill feeling
Joint stiffness
Muscle aches or joint pain
Night sweats
Prolonged fever
Sore throat
Swelling of the lymph nodes
Weakness
Loss of appetite
Weight loss
Since these are also symptoms of other illnesses, most people may not realize that they have been infected with CMV. If you have a pregnant patient experiencing symptoms similar to a seasonal illness, order a test for CMV IgM and IgG antibodies.
Signs of CMV infection in utero include the following:
Placental thickening
Organomegaly – abnormal enlargement of organs
Hepatomegaly – abnormal enlargement of the liver
Splenomegaly – abnormal enlargement of the spleen
Pyelectasis – dilation of the renal pelvis, the funnel-like dilated proximal part of the ureter (muscular tubes that propel urine from the kidneys to the urinary bladder) in the kidney (also a marker for Down Syndrome)
Megaloureter – abnormal dilation of the ureter
Ascites – a gastroenterological term for an accumulation of fluid in the peritoneal cavity (is a potential space between the parietal peritoneum and visceral peritoneum, that is, the two membranes that separate the organs in the abdominal cavity from the abdominal wall)
Fetal hydrops – accumulation of fluid in the fetal compartments
Abnormality of amniotic fluid
Microcephaly – small head circumference, more than two standard deviations smaller than average
Cerebral ventriculomegaly – dilation of the lateral ventricles of the brain
Intracranial calcifications – the build-up of calcium salts in the soft tissue of the brain
Hyperdense image in thalamic arteries
Periventricular echodensities
Hepatic echodensities
Intestinal echodensities
Cystic structures in the germinal zone
Signs/Symptoms of CMV in the Newborn
About 90 percent of babies born with congenital CMV will appear healthy at birth, and the vast majority will not have any visible symptoms or long-term issues. Many times, health problems or disabilities caused by congenital CMV infection can sometimes appear roughly two or more years after birth. Signs of CMV infection that may be present at birth:
Premature birth
Small size at birth
Small for Gestational Age (SGA)
Intrauterine Growth Restriction (IUGR)
Red or purple spots on the body caused by broken blood vessels (Petechiae / Purpura)
Yellow skin and eyes caused by increased bilirubin levels in the blood (Jaundice)
Liver problems
Lung problems
Spleen problems
Low blood platelet levels (Thrombocytopenia)
Small head size / small brain (Microcephaly)
Seizures
If your infant patient shows any of the signs and symptoms listed above, test the infant for congenital CMV infection using a saliva or urine PCR test. It is important to note that congenital CMV can only be accurately diagnosed if the newborn is tested within 21 days of life because, after 3 weeks, it is hard to determine if the baby could have contracted the infection through nursing or by exposure to siblings or others who may be shedding the virus. Please refer to the CDC for additional information regarding interpreting laboratory tests.
Treating Congenital CMV During Pregnancy
The Armstrong family.
If you have a pregnant patient who has been diagnosed with CMV during pregnancy, there are treatments and trials available. Recent studies indicate that Cytomegalovirus Immune Globulin Intravenous (CMV-IGIV) treatment may reduce the risk of congenital infection and/or disease in an unborn baby when given to pregnant women experiencing a primary CMV infection.
If you would like more information about clinical trials and the treatment options available to your patient during their pregnancy, please contact us.
Treating Congenital CMV in Newborns
Emerging research shows that antiviral drugs, Ganciclovir or Valganciclovir, may help newborns born with symptomatic congenital CMV. These antiviral treatments may prevent or lessen the severity of hearing loss and may improve head and brain growth. Ganciclovir and Valganciclovir can also help combat immediate medical concerns caused by CMV, such as thrombocytopenia, organ failure (most commonly spleen and/or liver), hepatitis, and pneumonitis. Treatments generally last from six weeks to six months and are administered orally or through an IV or PICC line.
Both Ganciclovir and Valganciclovir can have serious side effects, so be sure to consult with a doctor before and during the treatment period. Newborns receiving these antiviral treatments should have their regular blood counts taken to avoid problems with severe neutropenia or anemia.
If you have a newborn patient born with congenital CMV and you would like more information about antiviral treatments, please contact us. Ongoing Interventions & Therapies If you have a newborn patient diagnosed with congenital CMV, be sure to refer the patient to have their hearing and vision checked regularly to identify any early onset of hearing or vision loss. Early diagnosis is critical to experiencing long-term developmental successes.
If you are concerned about potential seizure activity in the newborn, ask the parent to record the baby’s behavior for your review. They may need to schedule a consult with a pediatric neurologist. Additional monitoring, including EEG, may be suggested to properly diagnose whether the child is experiencing seizures.
Refer your newborn patients born with congenital CMV to your local Early Intervention (EI) program to determine whether the child should be evaluated for EI services.
This information was provided by Farah Armstrong, founder of Maddie’s Mission and a co-founder of the National CMV Foundation. A graduate of the University of Texas, Farah has a Bachelor’s degree in Mechanical Engineering, with 10 years of work experience as an engineer with BP in Houston and a field development engineer with FMC Technologies in Singapore. When her daughter Madeline was born, they discovered she was severely affected by CMV, and she passed away after 12 days of life. In her honor, Farah began Maddie’s Mission. Her extensive engineering background gives her great expertise in planning, budgeting, and executing detailed operations, bringing together large groups of people from different backgrounds.
https://dandlelionmedical.com/wp-content/uploads/2022/06/Guide-Dimensions.png10051920dandywebhttps://dandlelionmedical.com/wp-content/uploads/2022/08/DandleLION-Logo-Color-800x278-1.pngdandyweb2022-06-21 12:28:242023-06-07 09:37:56A Silent Threat: CMV In Mothers and Babies
Infant positioning that mimics the intrauterine position positively impacts the healthy development of future motor milestones while having a substantial effect on the neurodevelopment of preterm infants. The DandleLION positioning system promotes the healthy development of the brain and body by more closely mimicking the womb, using the 5 Key Tenets of Neurodevelopmentally Supportive Positioning™.
Each of the 5 Tenets addresses a crucial aspect of intrauterine positioning. These tenets are the foundation of our FREE Positioning Competency Toolkit. We have created carousels for each tenet to provide a deep dive into what each tenet looks like when present, partial, or absent in infant positioning. Check them out below:
Flexion
Flexion in utero is vital to many biologic functions, including swallowing, digestion, joint development, calming, and self-regulation. In the NICU, positioning babies in a flexed posture aids healthy physical development and promotes calm. Flexion can be absent, partial, or complete.
Containment
The immature muscular development of the hospitalized preterm infant prevents them from self-perpetuating flexion, which is typically facilitated by the womb. Containment promotes a flexed posture and provides proprioceptive input, positively influencing the development of the brain and body.
Midline Alignment
Neutral alignment of the head, neck, and extremities along the midline promotes symmetrical musculoskeletal development, self-regulation, and calming.
360º of Proprioception
Proprioceptive input allows the infant to form neuronal connections that establish, to the developing brain, where the body lies in space. During gestation, the uterus encases the baby, providing proprioceptive feedback to the infant regardless of the way the infant moves or stretches.
In the NICU, proprioceptive input can be provided at varying degrees:
Absent or misplaced, with boundaries touching the baby but not in a way that provides proprioceptive feedback
Some proprioceptive input can be provided by boundaries around only the head or feet
Or ideally, 360 degrees of proprioception encases the baby, ensuring a feedback loop is provided to the baby with every movement
Free Movement & Recoil
The uterus allows for unrestricted movement and developmentally appropriate stimulation. Despite being an enclosed space with defined boundaries, there is freedom of movement that facilitates the development of proprioception. Using tools that provide gentle but dynamic resistance, regardless of the degree or direction of extremity extension, is essential to allowing the baby to move freely within the positioner while providing recoil to a flexed posture.
In the first example, a tightly swaddled hospital blanket does not allow for free movement and does not provide recoil
A simple positioning nest can allow free movement and may provide some recoil of the lower extremities, but the unsecured straps are unable to facilitate a return to flexion if they are loosened with startling
The ideal positioning support encircles the baby in a stretchy, responsive fabric covering that allows free movement and provides recoil, while promoting flexion, containment, and midline alignment and providing proprioceptive input
Learn more about how the Positioning Competency Toolkit can be utilized for your clinical practice by checking out our blog post or by downloading the Toolkit.
Dandle•LION is proud to partner with expert clinicians to provide the best available education and evidence-based care strategies. This month, we are excited to introduce you to Dr. Elizabeth Jeanson PT, DPT, CNT, DCS, NTMTC. Elizabeth is the Developmental Specialist and Neonatal Therapist in Neonatal Intensive Care at Sanford Children’s Hospital/USD Medical Center in Sioux Falls, South Dakota!
In her role as the developmental specialist, Elizabeth has the opportunity to implement developmental care protocols and practices for the unit and complete yearly developmental care quality improvement projects. In her role as a neonatal therapist Elizabeth is involved in direct patient care, family support, and education at the bedside.
Over the past 22 years, both Sanford Children’s Hospital and DuPont Hospital for Children have benefited from Elizabeth’s expertise and passion. Elizabeth completed NIDCAP training and Infant Behavioral Assessment certification. She is NeoNatal Neurobehavioral Scale (NNNS) and Neonatal Touch and Massage Therapy (NTMTC) certified, as well as being a certified neonatal therapist (CNT).
As a firm believer in sharing information and experiences, Elizabeth has presented nationally on topics including sensory development, positioning, nonpharmacologic pain management, change management, quality improvement, and Infant Driven Feeding™ Implementation. She is a NANT, Neonatal Touch and Massage, and Dr. Brown’s Medical lecturer.
Elizabeth has published two articles in peer-reviewed journals: One to One Bedside Nurse Education as a Means to Improve Positioning Consistency in 2013 and Applying the Four Disciplines of Execution to Promote Culture Change in the NICU in 2020. Currently, Elizabeth is formulating a change process mentoring system and working towards creative integration of trauma-informed care into the daily interactions with infants and families in the NICU.